Results
In the AGEhIV Cohort Study we identify various associated medical conditions, also referred to as comorbidities. Comorbidities become more frequent in the advancing age. Furthermore, we study the prevalence of risk factors for comorbidities and impaired organ functioning. Several analyses have been completed so far. We have examined which comorbidities occur more frequently in our cohort, and what risk factors are related to this increased frequency. This has also been examined separately for the different types of comorbidities and organ dysfunctions, such as cardiovascular diseases, arterial stiffness, high blood pressure, and bone density. In addition, we have studied frailty and participation in the labour market.
103 participants from the AMC and 78 participants from the GGD have participated in the neurological AGEhIV sub study. With the data collected in this sub study, we were able to look at the prevalence of neurocognitive (memory) impairment, the value of screening tests in predicting memory impairments, as well as retinal abnormalities of the eyes. Several other analyses are still ongoing.
Prevalence of comorbidities
Several studies have shown that different types of comorbidities occur more frequently among people living with HIV. In the AGEhIV Cohort Study, we study this topic extensively. The aim of the current analysis was to assess the prevalence of these comorbidities, and whether there is a difference between participants with and without HIV, with similar lifestyles. In addition, we were interested in identifying which factors are related to the prevalence of comorbidities.
During the first study visit all participants were asked to indicate whether they have had certain comorbidities in the past (e.g. heart attack, cancer or stroke). We verified this information by consulting either their hospital medical records in the case of participants with HIV, or by contacting their family doctors (GPs) in the case of participants without HIV. The presence of several other comorbidities was assessed by using blood pressure measurements (hypertension), lung function measurements, and blood tests (diabetes and hyperlipidemia) carried out during the first study visit.
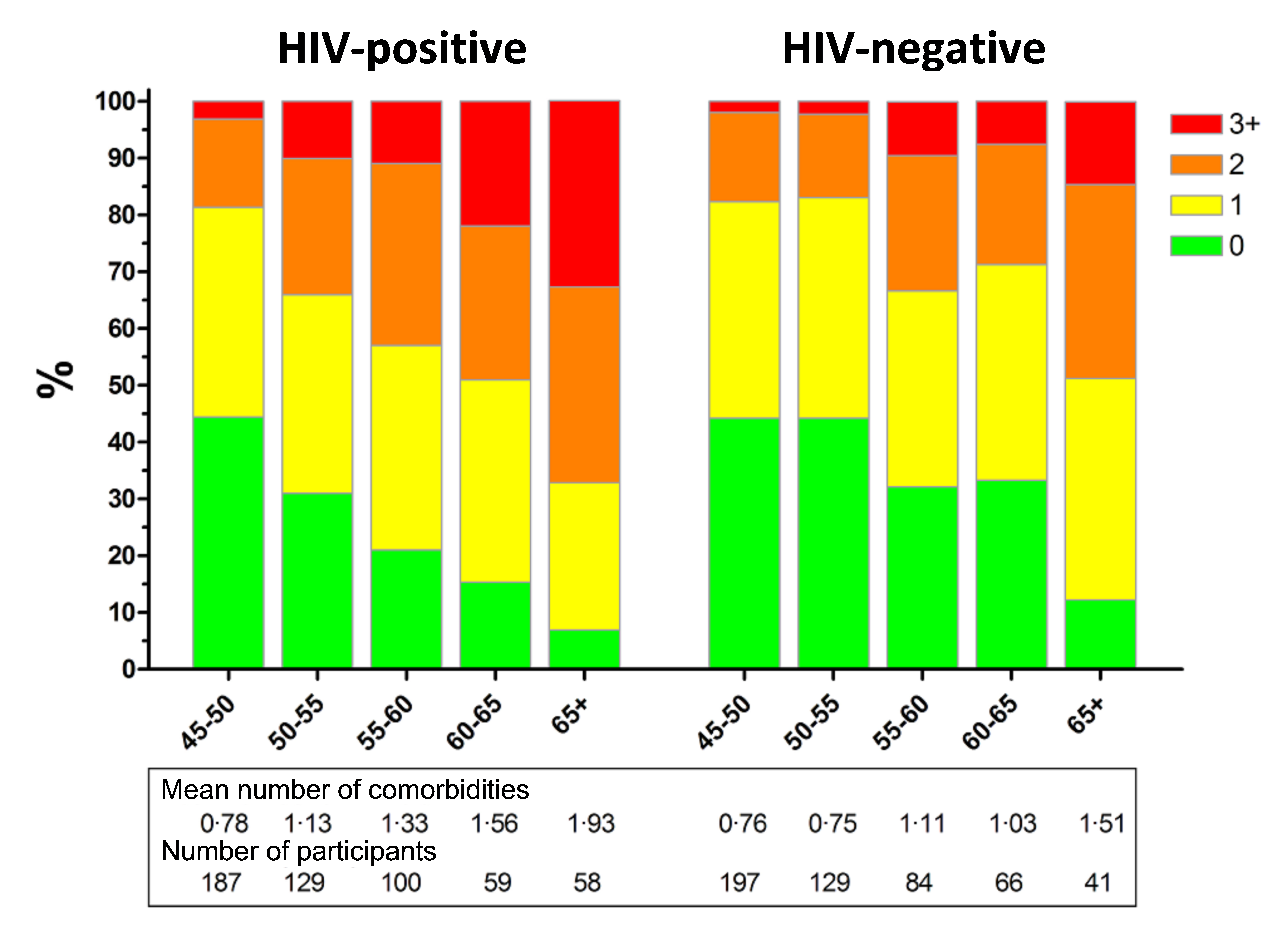
Figure 1
The analysis shows that participants with HIV on average had more comorbidities than participants without HIV (see Figure 1). The comorbidities that occur more frequently among people living with HIV are hypertension, myocardial infarction, peripheral artery disease in legs or abdomen and impaired renal function (see Figure 2). Our results suggest that having an HIV-infection is an independent predictor for having more comorbidities. Also, having had prolonged impaired immune function in the past (i.e. immunodeficiency defined as a CD4 count less than 200 cells per milliliter of blood), signs of a stronger inflammatory response measured in blood samples, and the use of high dose ritonavir (Norvir) were all separately associated with higher frequencies of comorbidities.
With the follow-up study visits, we aim to assess whether the differences in comorbidities between participants with and without HIV persist or increase even more, and which risk factors are related this difference.
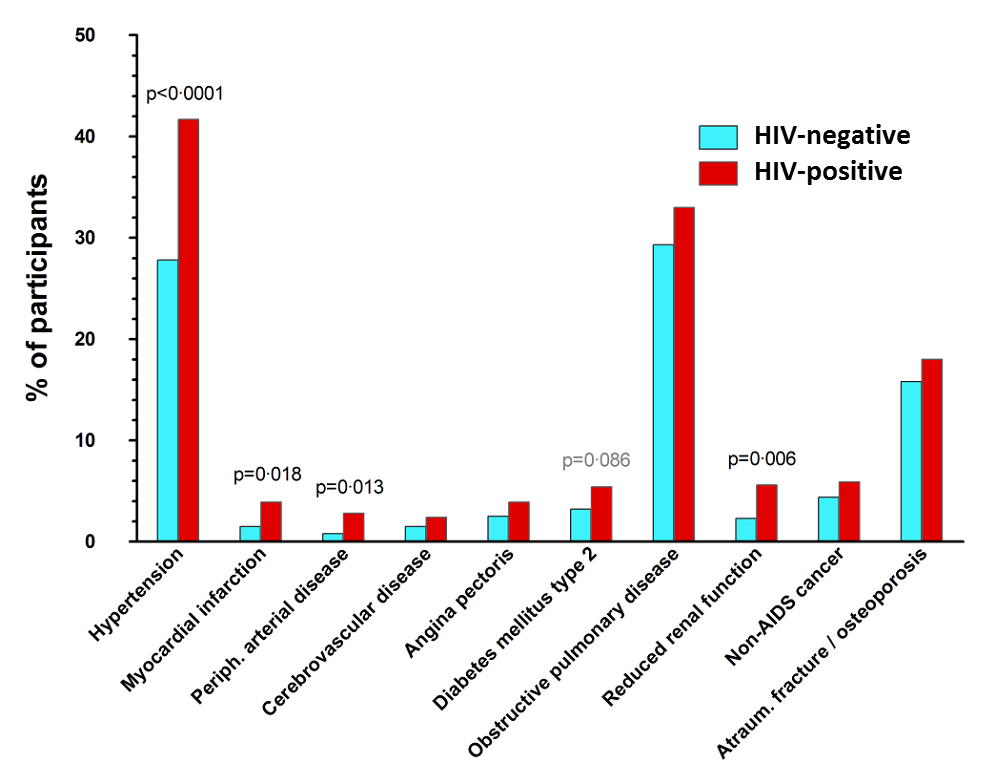
Figure 2
Learn more about this topic? Click here
Cardiovascular Disease
Various studies have shown that cardiovascular disease is common among people living with HIV. The AGEhIV Cohort Study has done extensive research regarding cardiovascular disease. All study participants have indicated in the questionnaire whether they have had a myocardial infaction, stroke, peripheral artery disease in legs or abdomen, or chest angina in the past. We verified the exact diagnosis in participants’ medical records (of the participants with HIV), or by contacting their GP (of the participants without HIV).
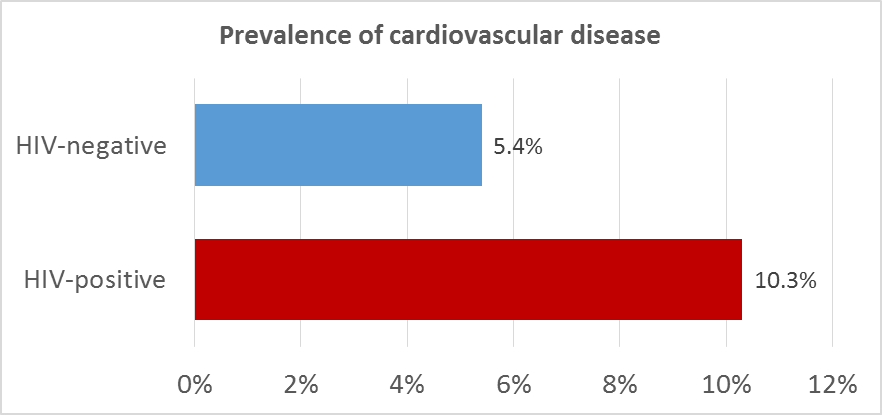
The results show that participants with HIV had a higher prevalence of cardiovascular disease compared to participants without HIV (see figure). There is strong evidence that having an HIV-infection is an independent predictor for having had cardiovascular disease, even after taking into consideration known risk factors such as smoking. Prolonged duration of immunodeficiency (CD4 count less than 350 cells per milliliter of blood) was independently associated with the prevalence of cardiovascular disease. In addition, prolonged use of ritonavir (Norvir) in a (nowadays no longer prescribed) high dose (400 mg/day) was associated with the prevalence of cardiovascular disease.
In the analysis, the role of AGEs has been studied in relationship with the prevalence of cardiovascular disease. AGEs (advanced glycation end products) are glycosylated proteins, which can accumulate in tissues. Older age, smoking, and inflammatory diseases lead to increased levels of AGEs. Participants with HIV on average had a higher AGE-value (2.4) than participants without HIV (2.1). The analysis also shows that the increased AGE-value might explain part of the increased prevalence of cardiovascular disease in participants with HIV. This could suggest that AGEs may play a vital role in the development of cardiovascular disease in people with HIV.
Arterial stiffness
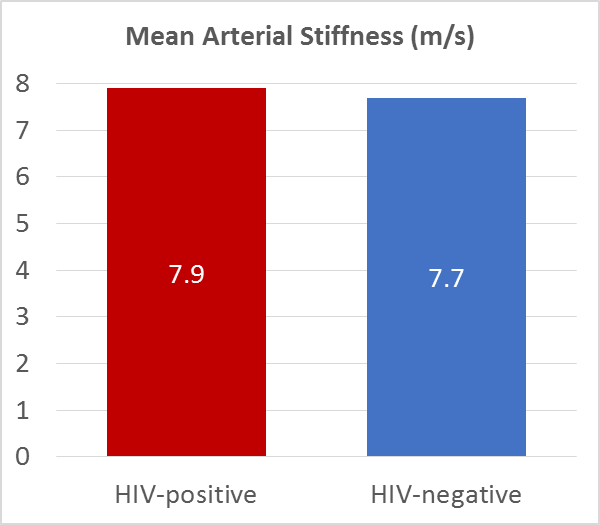
During the AGEhIV study visits the stiffness of the aorta has been measured in all participants using the Arteriograph®. The Arteriograph procedure is similar to a blood pressure measurement, and is performed using a cuff around the upper arm. The difference is that the cuff is more strongly inflated than during a conventional blood pressure measurement, in order to estimate the blood flow in the aorta. The stiffer the aorta is, the faster the blood flow. Aortic stiffness may indicate damage to the vessel wall, such as atherosclerosis. Increased arterial stiffness is related to an increased risk of cardiovascular disease.
In this study, we investigated whether arterial stiffness differs between participants with and without HIV, and aimed to identify factors related to an increased arterial stiffness.
Arterial stiffness measurements obtained in the first study visit showed that individuals with HIV had a slightly higher blood flow (and hence increased arterial stiffness) than individuals without HIV. However, the difference in arterial stiffness is very small: pulse wave velocity was 7.9 m/s in participants with HIV and 7.7 m/s in participants without HIV.
We hope to better understand the risk factors associated with increased arterial stiffness, and the relationship between arterial stiffness and the onset of cardiovascular disease through long-term follow-up of AGEhIV study participants.
The results also showed that cigarette smoking is a major risk factor for an increase in arterial stiffness. In addition, people with HIV who have had serious immune deficiencies in the past (i.e. CD4 counts below 100 cells per milliliter of blood) in particular had an increased aortic stiffness. This may indicate that these patients have an increased risk of cardiovascular disease.
Learn more about this topic? Click here
Hypertension
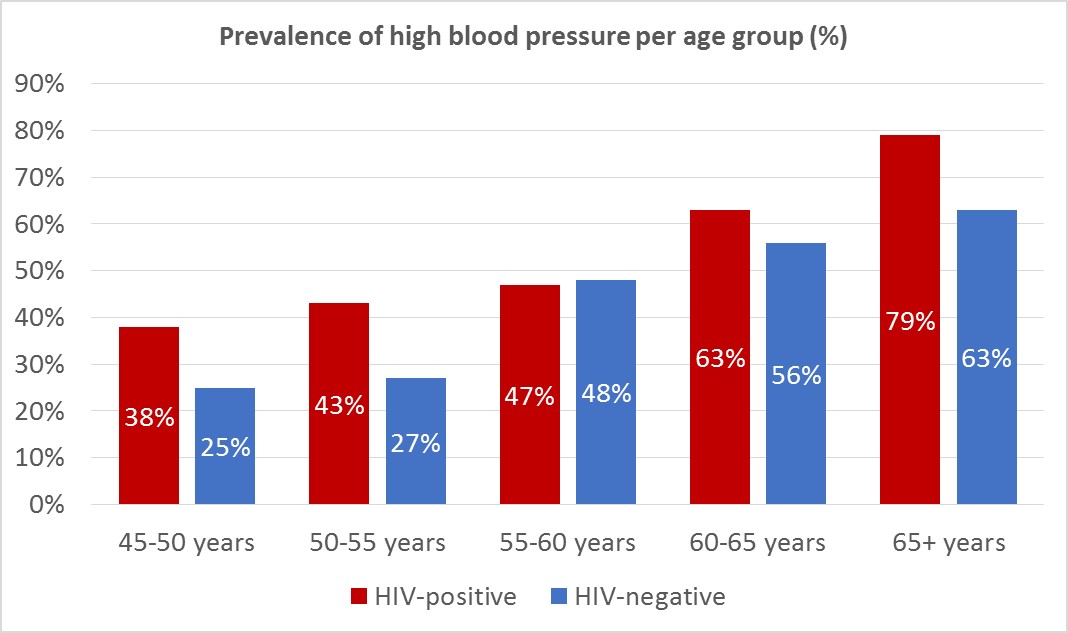
Hypertension (i.e. high blood pressure) is a major risk factor for the development of cardiovascular diseases. During each study visit blood pressure measurements were carried out in all participants, and use of antihypertensives was identified via a questionnaire. Based on this information, we have assessed the prevalence of hypertension in participants with and without HIV, as well as factors that were associated with the prevalence of hypertension.
Data obtained during the first study visit show that hypertension was more prevalent among participants with HIV in the AGEhIV Cohort Study (see figure).
Several factors play a role in the development of high blood pressure, including smoking, alcohol abuse, familial predisposition, insufficient physical activity, and obesity. The higher prevalence of hypertension among participants with HIV seemed mostly due to a larger waist-to-hip ratio in this group. This could partially be the result of the use of specific toxic antiretroviral drugs (stavudine) in the past.
We are interested to see whether there is an increase of the frequency of hypertension in participants with and without HIV in follow-up study visits.
Learn more about this topic? Click here
Bone Mineral Density
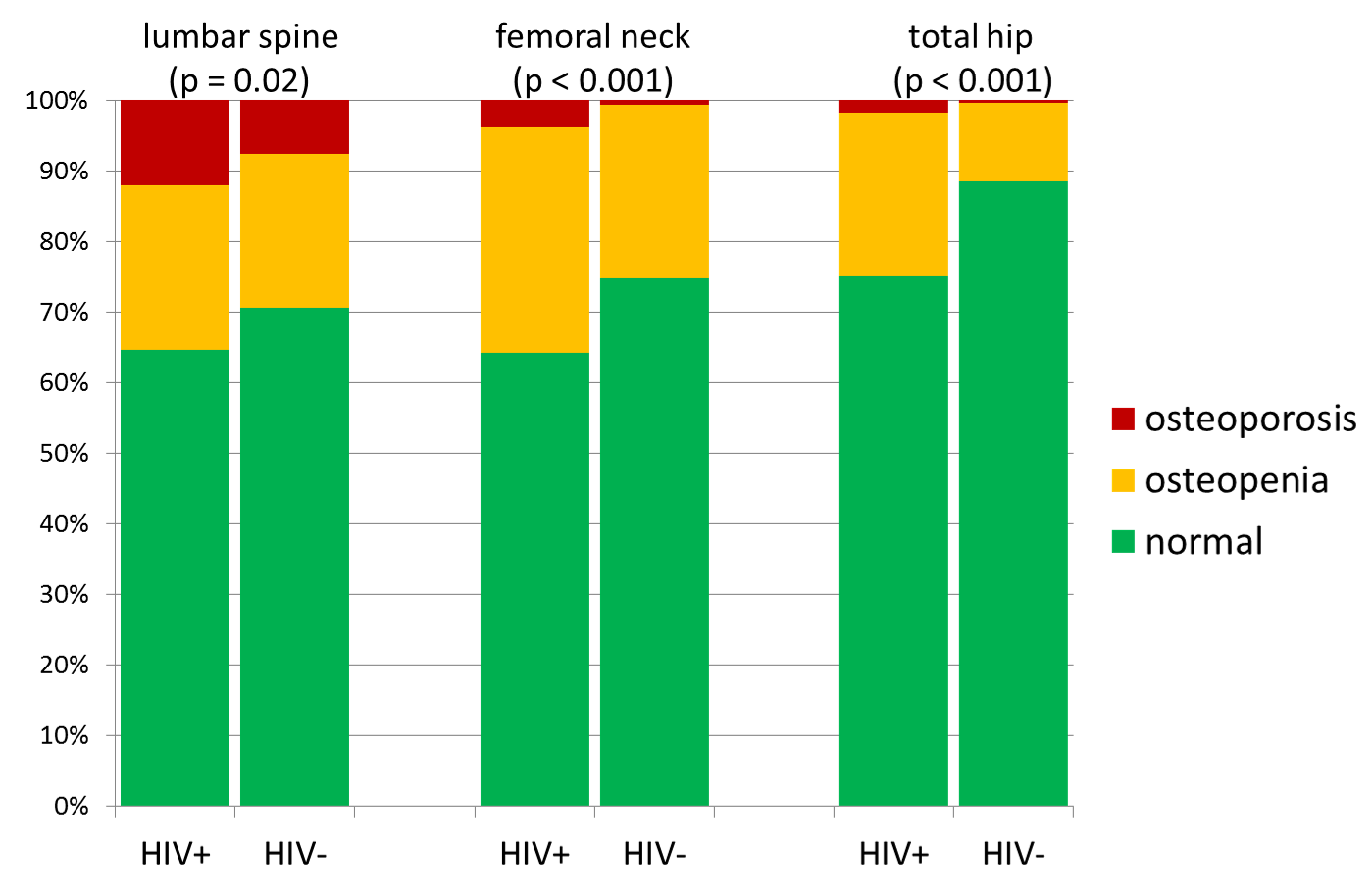
In all participants bone density was measured with the use of a DEXA scan. Bone density in the lumbar vertebrae (the lower spine), the upper part of the femur (upper leg bone) and the femoral neck were all measured. From the analysis of the measurements taken during the first study visit we found that osteoporosis (a greatly reduced bone density) and osteopenia (slightly reduced bone density) are both more common among participants with HIV in the AGEhIV Cohort Study (see figure). Osteoporosis can increase the chance of a fracture.
Two important risk factors for osteoporosis are a low body weight and cigarette smoking. It seems that the frequent occurrence of osteoporosis among the participants with HIV is mostly explained by the fact that a large part of the group smoked and had an – on average – lower body weight. The group that seems to face an additional risk is the group of participants with HIV who have previously gone through severe HIV diseases (such as AIDS) and currently have a lower body weight.
We are very interested to know the results of the following study visits, in which we hope to examine whether the change in bone density over time for participants with and without HIV is different.
Learn more about this topic? Click here
Frailty
All study participants answer questions during the study visits on unintentional weight loss. Also the pin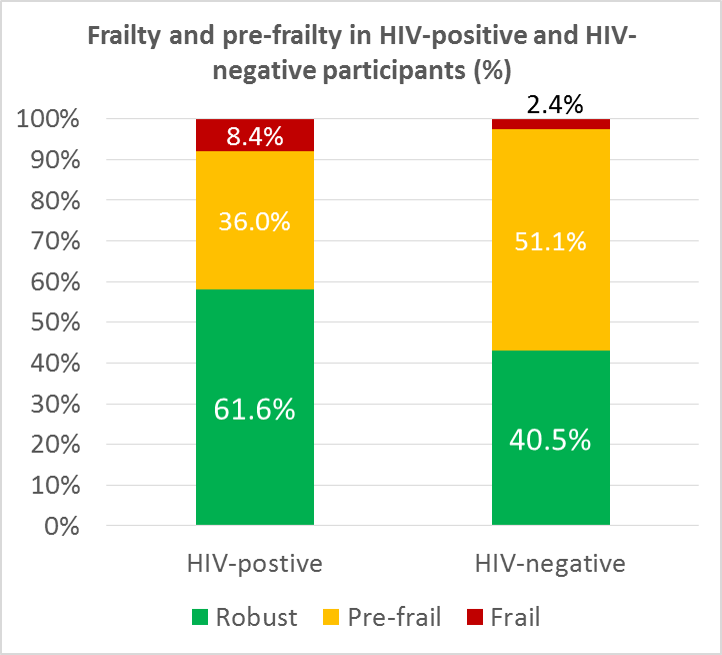 ching force of the writing hand and the walking speed is measured. Together these measurements are combined to determine if someone is “frail”, “pre-frail” or “robust” (not frail at all). In older people (65 years and over) it has been found that frailty is strongly associated with a risk of falling, hospitalization and death.
ching force of the writing hand and the walking speed is measured. Together these measurements are combined to determine if someone is “frail”, “pre-frail” or “robust” (not frail at all). In older people (65 years and over) it has been found that frailty is strongly associated with a risk of falling, hospitalization and death.
From the results of the first study visit it appears that study participants with HIV are more often frail or pre-frail (see bar chart). The relationship between HIV and frailty was independent of other factors that are also related to frailty. Our study showed some of these other factors to be older age, female gender, a chronic hepatitis C virus infection and symptoms of depression. All these conditions are independently associated with frailty. The results indicate that having more abdominal fat and less fat on the hips has been strongly associated with frailty. In people with HIV this can be a manifestation of the lipodystrophy syndrome associated with use of certain antiretroviral medication.
The precise meaning behind frailty in people with HIV, who are often younger, is not yet entirely clear. Regarding this subject, we hope to gain more knowledge during the follow up in the AGEhIV Cohort Study.
Learn more about this topic? Click here
Participation in the labor market
Although people living with HIV are living longer, there is evidence that this group faces age-related comorbidities earlier than people of the same age without HIV. This may have negative consequences for social participation, such as having a job. Among 885 participants of the working age (45-65 years) of the AGEhIV Cohort Study we have looked at the extent to which they participate in paid work, and if working, how their working functionality is.
We found that participation in paid employment was lower among participants with HIV (63.3%) than among participants without HIV (79.0%) (see Figure 1). This difference was largely due to a high percentage (21.7%) of participants with HIV that was completely unable to work. (see Figure 2).
Important factors contributing to being able to participate in paid work were older age, having multiple comorbidities (illnesses) and experiencing stigmas on the workflow.
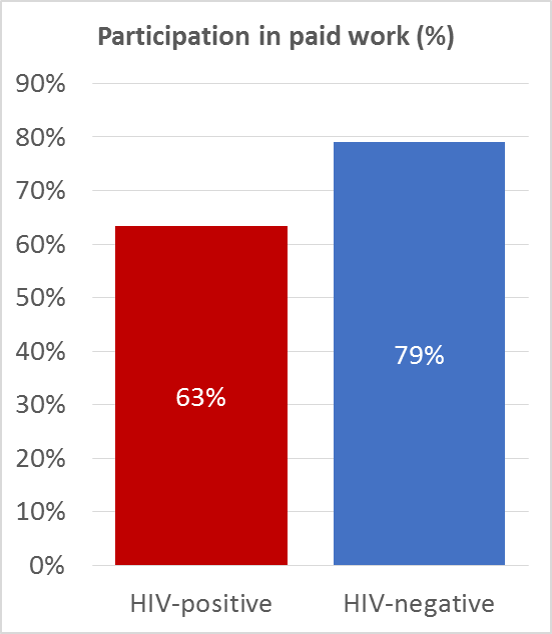
Figure 1
Among the working participants, we also examined their working capacity; a measure of how well a person can perform in his job. Participants with and without HIV reported the same level of working capacity. This suggests that those living with HIV who did not already have to stop working due to illness, will perform similar to those without HIV.
A diminished working capacity is often reported by those – for example – who have little flexibility to deal with recovery from illness at their workplace, such as being able to plan working hours or holidays freely. Additionally, I appears that having a lower working capacity is also related to having larger work related fatigue and more absence due to illness. People with symptoms of depression, having a part-time job and those born outside of the Netherlands also report lower working capacities.
Learn more about this topic? Click here
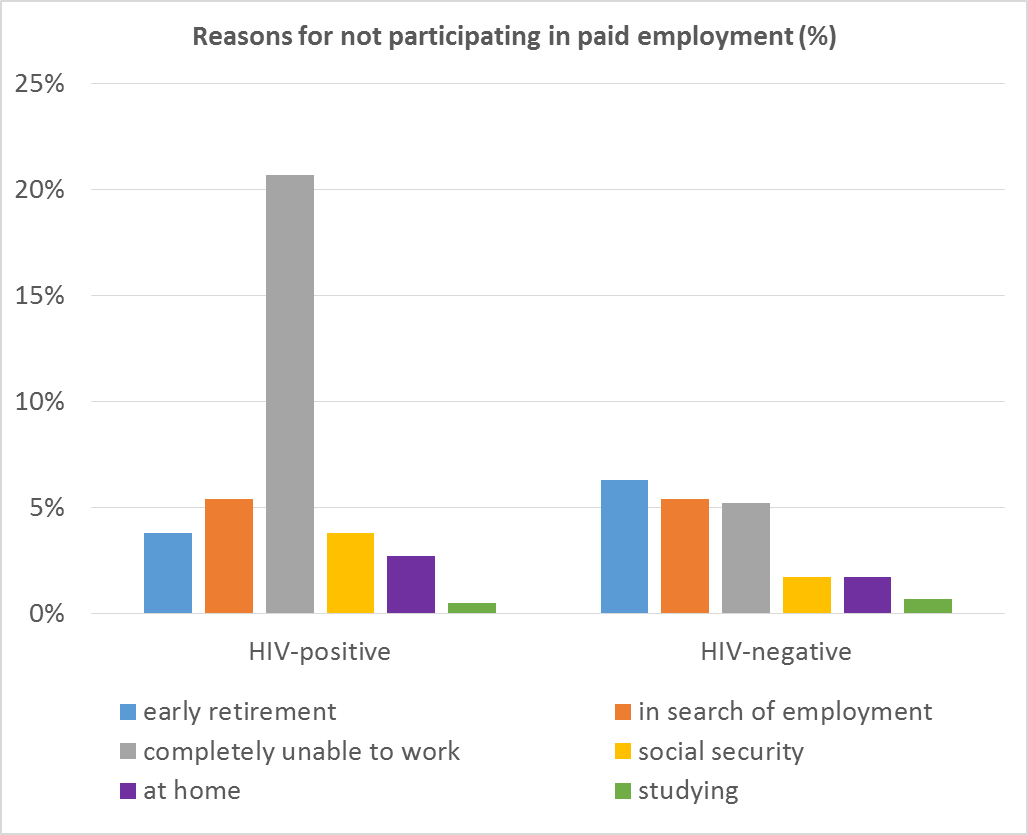
Figure 2
Prevalence of cognitive impairment
Before the introduction of antiretroviral therapy, AIDS dementia was one of the most feared complications that could occur as a result of advanced HIV-infection. Despite the currently highly effective treatment for HIV, mild memory impairments (HAND) still seem to be associated with having an HIV-infection. The exact extent of this association remains unclear, as memory disorders occur in both people with and without HIV and could be related to multiple other risk factors as well.
All participants of the AGEhIV neurological sub study underwent a comprehensive neuropsychological assessment. During this assessment six different domains were examined: speech, attention and information processing speed, as well as executive, memory and motor functions.
Results of participants with HIV were then compared with results from participants without HIV with similar age and educational backgrounds. Hereby we determined whether a person was performing below expected levels or not and if the participant could be classified as having HAND (HIV-associated neurocognitive disorders). This classification can be performed in different ways. In the current study, we classified participants using the Frascati criteria, Gisslen criteria and the MNC method.
The estimated occurrence of HAND varies greatly depending on the classification method used. However, whichever method used, results show that HAND is more prevalent among participants with HIV (see figure). After the second study visit, we also hope to make a more elaborate statement about the occurrence of HAND over time.
Learn more about this topic? Click here

Quality of Simple Memory Tests for the Diagnosis of Cognitive Impairment
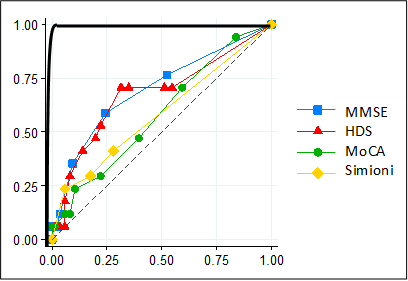
A perfectly reliable (hypothetical) screening test is represented by the black line. A completely unreliable (hypothetical) screening test is represented by the dotted line. A real-world good screening test will therefore resemble the pattern of the black line more closely than that of the dotted line.
A screening test is a test that is used to trace down people with a particular disease or condition in a large group of people. In the case of cognitive impairment a screening test could be used to identify those at increased risk for developing cognitive impairment. People that screen positive could then be examined more extensively by means of a complete neuropsychological examination. A good screening test has to meet certain requirements. The central question in this analysis is to determine to what extent some of the commonly used screening tests for memory deficits meet the requirements for identifying those at risk for HIV-associated neurocognitive disorders (HAND).
In the AGEhIV Cohort Study four different screening tests were studied: HDS (specifically developed for HIV dementia), Simioni questions (consisting of three questions that have been used in trials in mild HIV-associated neurocognitive impairment) MoCA and MMSE (two tests commonly used to screen for other forms of dementia, for example in Alzheimer’s Disease). The results of these screening tests were compared to the results from the extensive neuropsychological assessments performed within participants of the neurological sub study. All screening tests performed moderately to poorly when comparing them with the extensive neuropsychological assesments (see figure). The four screening tests are therefore unreliable and not sufficient to identify HAND, thus not useful for screening in clinical practice.
Learn more about this topic? Click here
Eye examination

Photograph of the retina
Former studies have suggested HIV causes premature aging of the retina. Within an AGEhIV sub study we performed an ophthalmic examination consisting of a number of function tests (e.g. measurement of the contrast sensitivity) and a number of imaging studies of the retina.
All participants have completed their first eye examination and the results have been analyzed. In conclusion, we found no differences in the structure or function of the retina between those with and without HIV. This is good news for the participants with HIV, as a well-suppressed HIV infection seems to prevent changes to the retina.
Treatment of cardiovascular disease and its risk factors
At each study visit, we ask participants whether they have developed cardiovascular disease, for example whether they have had a stroke or a heart attack. We also evaluate whether the participants have risk factors for cardiovascular disease, such as high cholesterol levels, high blood pressure, or smoking. Using this information, we have been able to compare whether cardiovascular disease or its risk factors occur more often in people with HIV than in people without HIV. Moreover, we evaluated whether participants were appropriately treated for cardiovascular disease and the associated risk factors. Treatment of cardiovascular disease risk factors, such as the use of antihypertensive drugs to reduce blood pressure to normal levels, is important to reduce the risk of a new cardiovascular event.
At the first study visit, cardiovascular disease was more prevalent in participants with HIV than in participants without HIV (10% and 5%, respectively). Among the participants with no history of cardiovascular disease, we evaluated the risk of developing cardiovascular disease in the next 10 years. We calculated this risk based on the presence or absence of certain cardiovascular disease risk factors. We found that participants with HIV were more likely to have a high cardiovascular disease risk than people without HIV (figure 1). The most frequently-observed risk factors for cardiovascular disease were insufficient physical activity, smoking, high cholesterol levels, and high blood pressure. These risk factors were more common among participants with HIV.
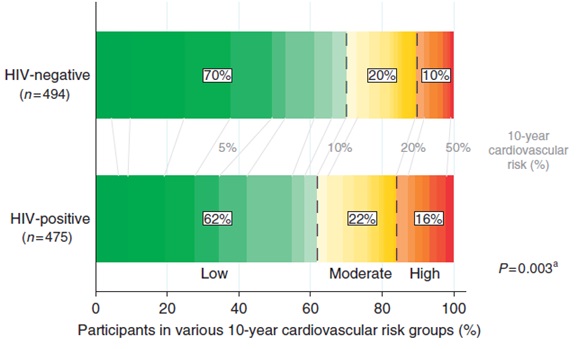
Figure 1. Estimated 10-year cardiovascular disease risk among participants with and without HIV who had no history of cardiovascular disease.
When evaluating whether participants have been adequately treated for their cardiovascular disease risk factors, we focused on those participants at high risk of a cardiovascular event (i.e., those participants who had a history of cardiovascular disease or a high estimated cardiovascular disease risk due to a combination of several risk factors). We found that approximately half of these “high risk” participants had high blood pressure, which, in the majority of the cases, were not being treated with antihypertensive medication. Moreover, over 60% of the “high risk” participants had elevated cholesterol levels, which, in the vast majority of cases, were not being treated with lipid-lowering medication. No significant differences were observed between people with and without HIV.
Next, we focused on participants who used medication to treat high blood pressure or high cholesterol. Approximately 50% of these individuals had optimal blood pressure and cholesterol levels (figure 2). Again, no significant differences were observed between people with and without HIV. However, we did observe that people with HIV who had a history of cardiovascular disease were more likely to use anticoagulant or antiplatelet drugs than people without HIV (85% versus 63%).
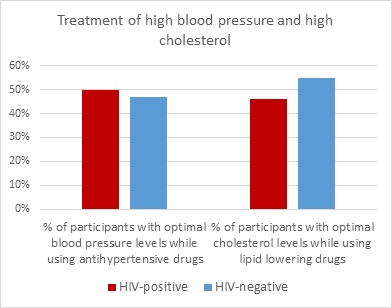
Figure 2: Percentage of participants who have optimal blood pressure/cholesterol levels while using medication for a high blood pressure/cholesterol.
This study shows that treatment of cardiovascular diseases and associated risk factors is suboptimal, both in people with and without HIV. To prevent cardiovascular disease, a healthy lifestyle and adequate treatment of risk factors for cardiovascular disease are important and therefore require the attention of both patients and their doctors.
Chronic Kidney Disease
At each study visit, we take blood samples and ask study participants to provide a urine sample. We use this material to study kidney function and to look for indications of kidney damage in people living with HIV and those without HIV.
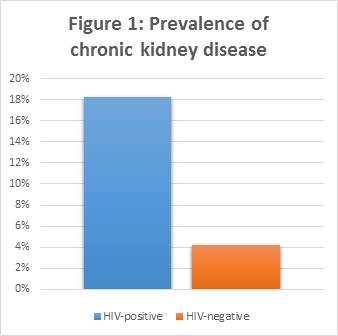
By looking at the levels of albumin in the urine and the levels of creatinine in the blood, we can detect the presence of a reduced kidney function. Our results showed a higher frequency of chronically reduced kidney function in people with HIV compared to people without HIV (figure 1).
In addition, we studied the course of kidney function over 4 years of follow-up. Kidney function declined in all participants, but we found a stronger decline in people living with HIV (figure 2).
There are several possible explanations for the poorer kidney function observed in people with HIV. First, there are several drugs against HIV (antiretroviral drugs) that are known to have a negative effect on kidney function. One of these is the frequently-used drug tenofovir. Tenofovir is used, or has been used, by a large proportion of the individuals with HIV in the AGEhIV Cohort (73% and 12%, respectively).
It remains unknown whether tenofovir use causes a more rapid decline in kidney function. Our study found no compelling evidence to support this theory. However, since such a large proportion of study participants with HIV use tenofovir, we cannot rule out such an effect. To investigate it further, we would need a comparable group of people with HIV who have never used tenofovir. Unfortunately, we do not have such a group in our cohort.
The results of our study do, however, confirm that traditional risk factors, such as cigarette smoking and hypertension, contribute to a decreased kidney function in people with HIV. Moreover, poorer kidney function in people living with HIV may be due to higher levels of inflammation, which are known to persist in people with HIV despite adequate treatment of their HIV infection.
The older version of tenofovir (disoproxil fumarate tenofovir; TDF) is now frequently being replaced in many HIV treatment regimes by a newer version, namely tenofovir alafenamide (TAF). TAF has fewer negative effects than TDF, including less kidney damage.
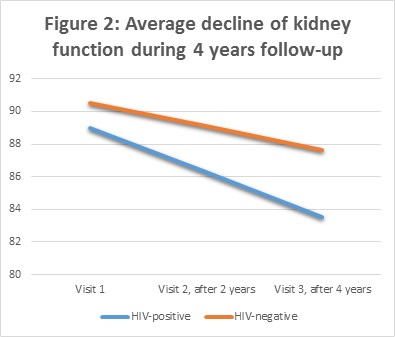
Renal function is expressed in milliliter per minute (ml/min)
Cigarette smoking and inflammation
Cigarette smoking increases the risk of cardiovascular disease and premature death. Some studies have suggested that the negative effects of smoking may be worse in people living with HIV than in people without HIV.
People living with HIV and people who smoke are more likely to have elevated levels of several markers of inflammation. It is thought that this type of chronic inflammation could lead to earlier onset of age-related illnesses, such as cardiovascular disease. In the AGEhIV study we therefore compared the levels of four of these inflammatory markers in the blood of smokers compared with those in non-smokers. In addition, we evaluated whether smoking has a stronger effect on the levels of these markers in people with HIV than in people without HIV.
The markers we studied were C-reactive protein (CRP), D-dimer, sCD14, and sCD163. CRP is a general marker for inflammation in the blood and D-dimer is a marker for activation of the blood coagulation system. sCD14 and sCD163 are both markers for activation of monocytes, a specific type of white blood cell. Monocyte activation and coagulation may play a role in plaque formation, which may cause cardiovascular disease.
We found higher levels of CRP, D-dimer, and sCD14 in cigarette smokers, regardless of their HIV status. These elevated levels of inflammatory markers likely contribute to the negative health effects of cigarette smoking. We also found higher levels of CRP, sCD14, and sCD163 in people with HIV than in people without HIV, regardless of their smoking status. We found no evidence of smoking having a more marked negative effect on inflammatory markers in people with HIV.
At present, it seems that the reported additional negative effects of smoking on the health of people living with HIV cannot be explained by smoking having a stronger effect on either inflammation or blood coagulation. Further studies are therefore needed to explain this effect.
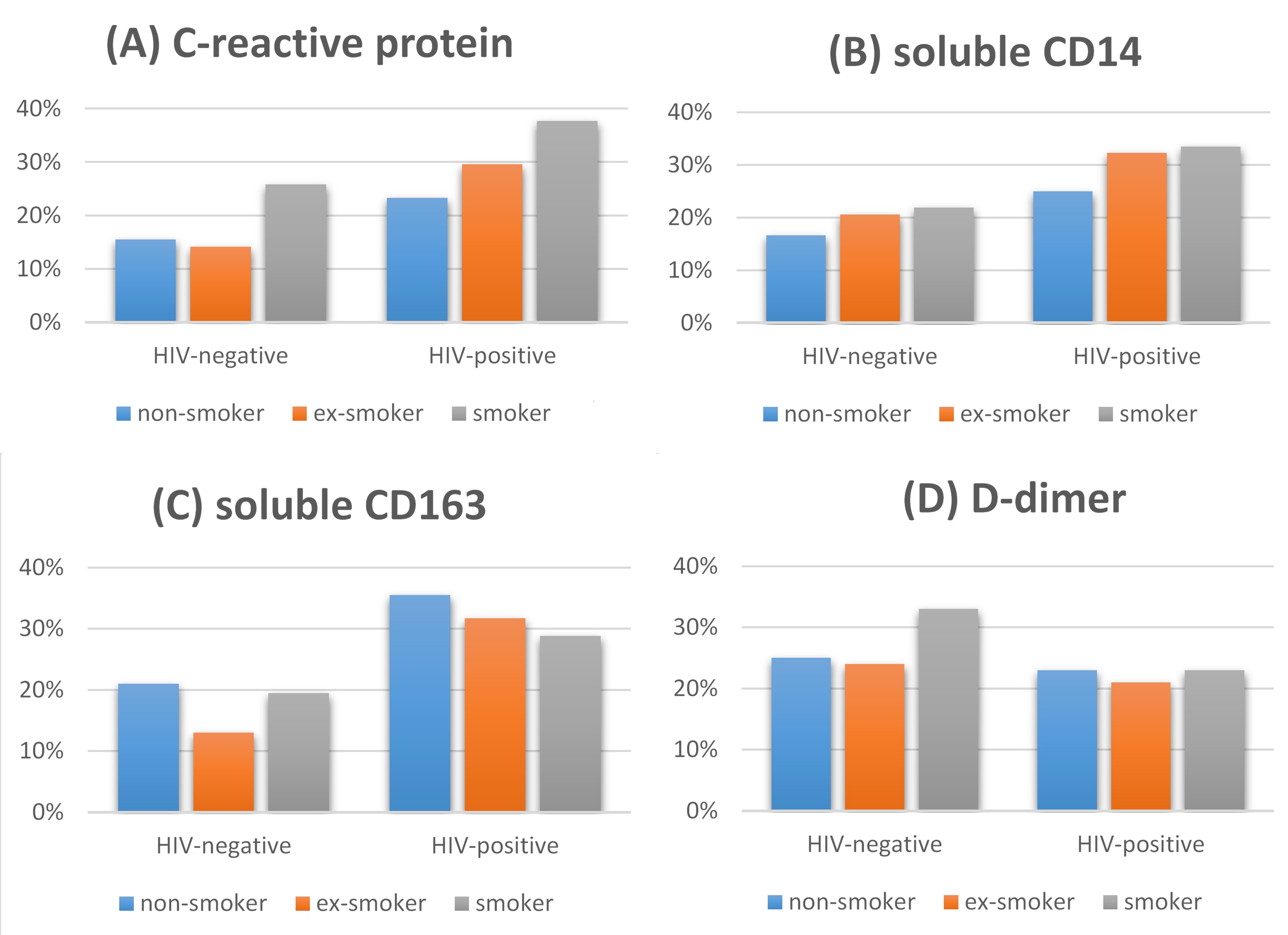
Proportion of people with a high level (i.e., a value in the upper quartile) of the following markers: C-reactive protein (A), soluble CD14 (B), soluble CD163 (C), D-dimer (D)
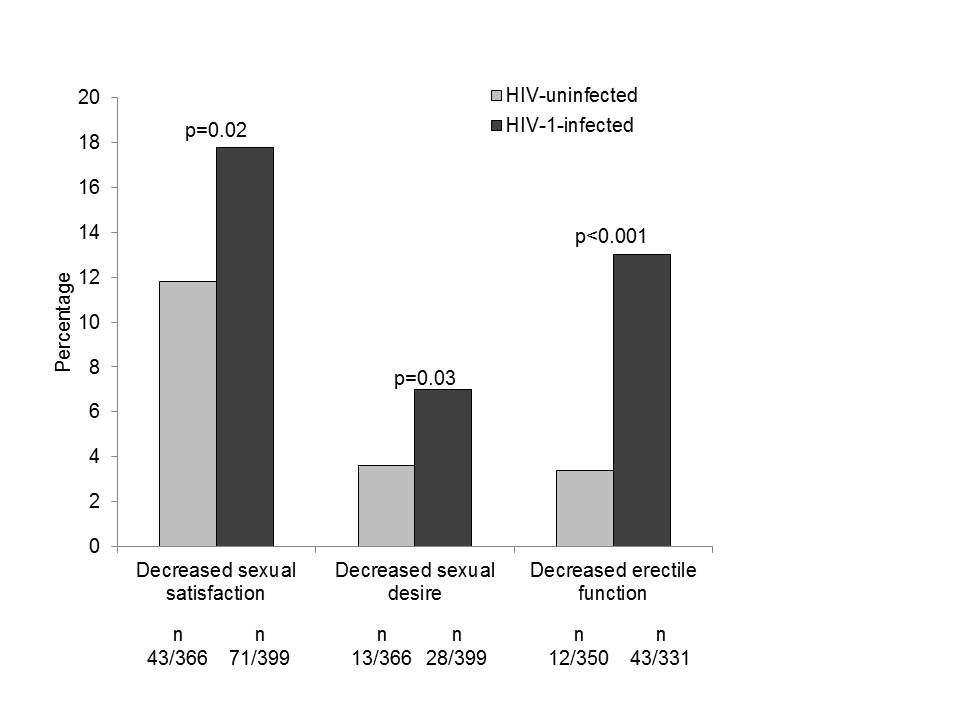
Sexual function
In this analysis we assessed whether people living with HIV experience more sexual problems than people without HIV. The questionnaire which participants complete at each study visit includes questions about sexual functioning. We assessed what men who reported having sex with men had answered to these questions. The questions concerned three sexual domains: erectile function, sexual satisfaction and sexual desire. The responses to these questions revealed that men having sex with men living with HIV experienced decreased erectile function, decreased sexual satisfaction and decreased sexual desire more often than their counterparts without HIV. This could partly be explained by the fact that the men living with HIV more often reported depressive symptoms, had more other diseases and more often used medication for high blood pressure – each of which are all also related to sexual functioning. The difference in erectile function (getting an erection) was most pronounced between the men with HIV and without HIV. Those who were treated for HIV with lopinavir/ritonavir (Kaletra) in the past or at the time of their first study visit more often experienced decreased erectile function. Based on these results, we have expanded the number of questions on sexual functioning in the study questionnaire, so that we can evaluate sexual functioning among study participants in more detail in the future.
For more information, click here
The development of comorbidities over time
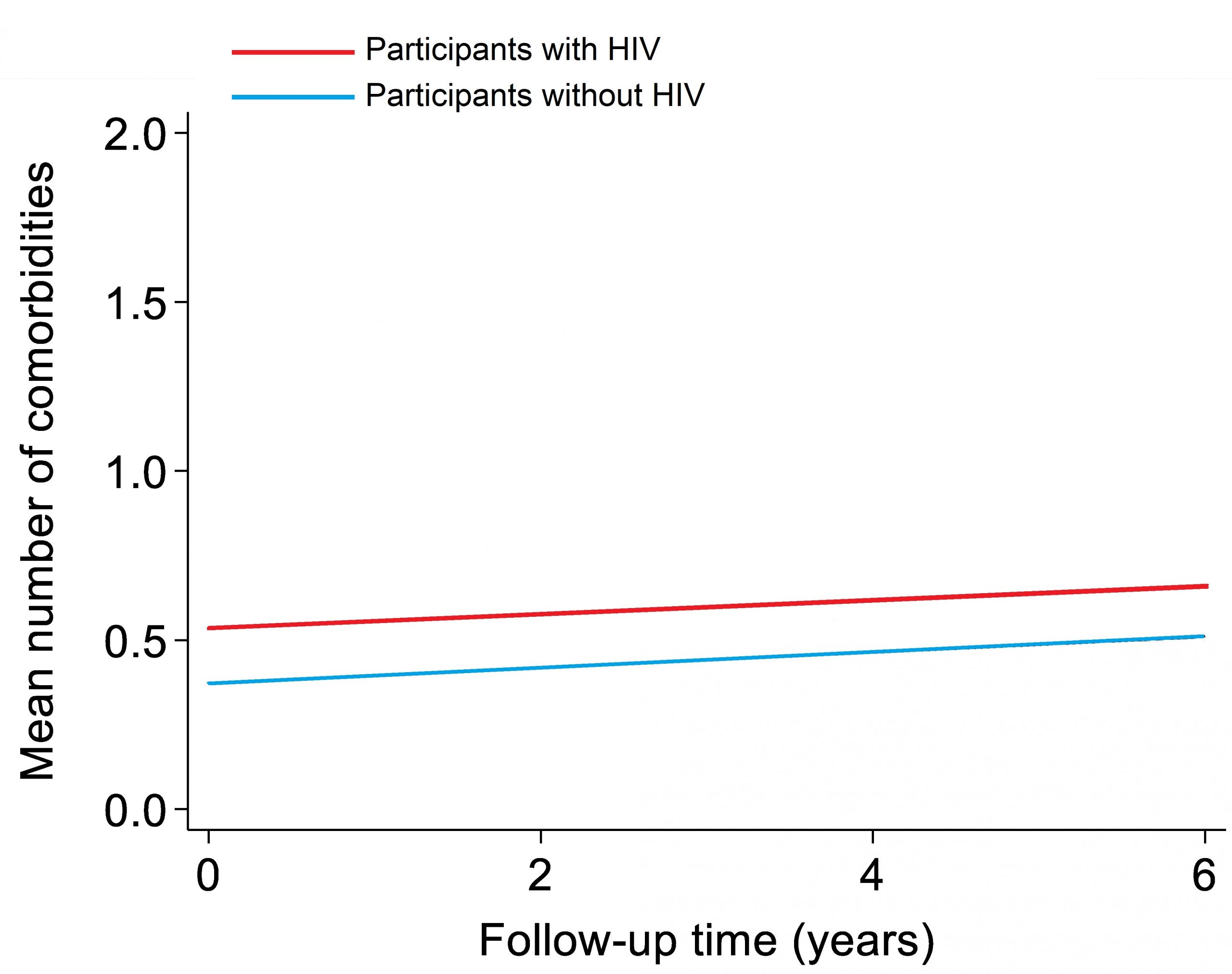
The main aim of the AGEhIV Cohort Study is to answer two questions. Firstly: do people with HIV develop additional diseases, so-called comorbidities, more quickly than people without HIV? And secondly: which risk factors play a role in this? Earlier research in our study already showed that participants with HIV do indeed have more comorbidities on average than participants without HIV. The comorbidities that are more common among participants with HIV are high blood pressure, myocardial infarction, narrowed blood vessels of the legs or abdomen, renal impairment, and reduced lung function. Until now it was unclear whether the difference in the number of comorbidities between participants with and without HIV increases over time as participants get older.
We have now investigated this by looking at the change in the average number of comorbidities. We compared this between participants with and without HIV over a six-year period. At the first study visit, the average number of comorbidities was higher in participants with HIV than in participants without HIV. Over time, participants from both groups developed more comorbidities. This increase was equally rapid in participants with and without HIV. This can be seen in figure 1: the red line (participants with HIV) starts and remains higher than the blue line (participants without HIV), but the lines rise at the same rate.
Figure 1
The risks associated with these comorbidities were also examined. It turned out that people with more comorbidities had a higher risk of dying. This higher risk of death was mainly due to cancer. This did not concern the cancers typical of AIDS (Kaposi’s sarcoma, certain types of non-Hodgkin’s lymphoma, and cervical cancer), but other cancers (such as lung, colon, anus, and liver cancer).
What does this mean?
The results of this study are partly reassuring. People with HIV who use successful antiviral treatment do not develop comorbidities at an accelerated rate as they age compared to people without HIV. So even though people with HIV had more comorbidities at the time the study started, the difference in comorbidities compared to people without HIV did not increase. Nevertheless, it remains important to prevent these comorbidities, to detect them at an early stage and to treat them in time. This certainly applies to the ‘non-AIDS-related cancers’ as well.
Do you want to know more? Click here for the article.
Cardiac autonomic control
It has been known for some time that people with HIV have an increased risk of cardiovascular disease. Partly, this is due to general risk factors for cardiovascular disease such as smoking, obesity, high cholesterol, diabetes and sometimes hereditary factors. We also know that the presence of HIV plays a role. HIV causes chronic inflammation in the body, which remains present even with good use of HIV medication. From research among the general population, we know that chronic inflammation can disrupt the control of the nervous system on the cardiovascular system (this is also called cardiovascular autonomic control). And that this increases the risk of cardiovascular disease.
We measured cardiovascular autonomic control in all AGEhIV Cohort participants between 2016 and 2018 with a 10-minute blood pressure measurement. We compared the results of this measurement between AGEhIV participants with and without HIV. We know that these two groups do not differ greatly in terms of lifestyle factors that are known to increase the risk of cardiovascular disease. To investigate the role of lifestyle, we also compared the measurements in our participants with those in participants of the HELIUS (HEalthy LIfe in an Urban Setting) study, who reflect the general Amsterdam population. We specifically looked at men between 50 and 70 years old of European descent to make the comparison between the groups as reliable as possible.
The study found that European male AGEhIV participants with HIV aged 50 to 70 years had, on average, slightly worse cardiovascular autonomic control than both AGEhIV participants without HIV and HELIUS participants. Among participants with HIV, men who had previously had more impaired immune function due to HIV (as determined by lowest CD4 count ever) now appeared to have more impaired cardiovascular autonomic control. This also applied to participants who had used the HIV medications stavudine, didanosine, zalcitabine or zidovudine in the past (and especially for a long period of time). Our results suggest that impaired cardiovascular autonomic control could be one of the explanations for the increased risk of cardiovascular disease we see in people with HIV.
For more information, click here